
Critical Care or Overlooked? Struggles in Saskatchewan’s Primary Care on Reserves and Remote Communities
Contributors: Andrea Vera, Deborah Adedayo, Joshua Potter, Xander LeClaire, Connolly Gamble

A view of the Pasqua First Nation sign. Photo by Andrea Vera
Reighlene Peigan grew up on Pasqua First Nation, Saskatchewan, alongside her mom, her brother, her three cousins, her niece and her daughter Brielle, who is now 8 years old.
She understands firsthand how difficult it can be to maintain your health when you don’t have a family doctor.
“It's pretty tough, especially when you have small kids that are super, super sick, even to get medicine and stuff like that, it's a struggle,” says Peigan.
Peigan does not have a family doctor, neither does her family. There isn't a family doctor on her reserve, making misdiagnosis and lack of continuous care part of her everyday reality.
In 2023, she moved off the reserve and into Regina due to the lack of housing.
Now, at 26-years-old, Peigan still feels the consequences of a system that lacks primary care, especially when trying to take care of her young daughter.
On the reserve, even basic healthcare was very hard to access. “It wasn’t the best,” says Peigan, “the nearest doctor was in Fort Qu’Appelle.”
The distance is not only an issue for those who struggle with the commute, but it often makes severe illnesses difficult to diagnose and treat.
Peigan says a good example of this is her own grandfather. For months, doctors treated her grandfather for a lung infection.
“They just kept giving him antibiotics… until it was super, super progressed,” says Peigan. Her grandfather was later diagnosed in Regina with stage three throat cancer.
Efforts to improve access to care are ongoing, but gaps remain.
“Reserves have health centers, but they only have nurses that work there, like maybe once or twice a week,” says Peigan. “Just because of the lack of nurses, lack of doctors.”

A rural view of on reserve communities where healthcare access remains a struggle. Photos by Andrea Vera.
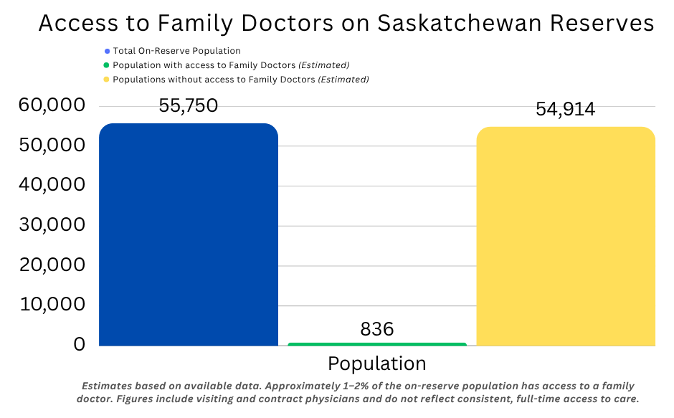
In Saskatchewan, the total Indigenous population is distributed among 75 First Nations, and consists of 187,890 people. Approximately 47.8 percent, or 53,010, live on reserve, while 52.2 percent, or 97,830, live off reserve
It is estimated that only 1 to 2% of the people living on reserve have access to a family doctor.
Dr. Udoka Okpalauwaekwe, a physician and primary care researcher at the University of Saskatchewan, says consistent access to health care becomes more impossible every day.
“Saskatchewan has a recruitment system, but a serious retention problem,” says Okpalauwaekwe.
Since 2011, more than 600 internationally trained physicians have been brought into the province through the Saskatchewan International Physician Practice Assessment Program (SIPPA).
“Out of those 600, 83 per cent have left the province,” says Okpalauwaekwe. “We’re always recruiting,” he adds. “But we’re losing more than we’re recruiting.”
While an estimated 52 to 57 per cent of physicians work in urban areas, only about 47 per cent serve rural Saskatchewan, despite the province’s geography and population needs.
Despite those numbers, there are no doctors on reserve. Access is limited mainly to emergency rooms and walk-in-clinics in nearby communities.
“We don’t have figures,” says Okpalauwaekwe. “We can only extrapolate, I would say one to two per cent.”
Saskatchewan has about 2,644 physicians in total, including 1,442 family physicians, but distribution remains uneven, with about 55 per cent in urban areas, 25 per cent in rural settings, and 20 per cent in smaller cities.
Healthcare on reserve is delivered through a different model, where nurses are in charge of primary care while family physicians supervise remotely.
Healthcare is also coordinated through federally funded organizations such as the Northern Inter-Tribal Health Authority (NITHA), alongside community-controlled models and organizations like Northern Medical Services.
The division between organizations creates fragmentation, making centralized oversight of patients almost impossible.
Patients often lack continuity of care, meaning they do not have consistent access to providers who know their medical history, coordinate treatment, or build long-term trust. Access to a family doctor would allow for earlier diagnosis, better coordination of care, and stronger patient and doctor relationships.
Peigan experienced this fragmentation of health care with her daughter.
“Going doctor to doctor, having to repeat yourself and repeat the information,” says Peigan. “You're trying to explain the best you can medically to an actual doctor, that's pretty tough.”
Peigan, who grew up on Pasqua First Nation, says her daughter struggled with pneumonia every winter. It took them 8 years to get a formal asthma diagnosis.
“She has an inhaler now,” says Peigan. “I think, had she been diagnosed with her asthma earlier, she wouldn't have had pneumonia every winter.”
Okpalauwaekwe points to deeper structural issues in how care is organized. “The system is designed so that family physicians are the gatekeepers of care,” he says. “If you want to see a specialist, you have to go through them first.”
In Saskatchewan, the Northern Medical Services (NMS) is the organization responsible for providing health services across northern and remote communities.
The director, Dr. Veronica McKinney, says delivery is already built on a model that challenges how the rest of the province still operates.

Dr. Veronica McKinney. Photo contributed by Shalayne Hendriks, Executive Admin Support to Dr. McKinney.
“We provide medical services, but our mandate is broad. Primary health care, health promotion, specialist care, public health, education, research, ” says McKinney.
“In the 2024–25 fiscal year, we had 2,782 clinics and 51,102 patients seen,” McKinney added.
Their reach goes beyond primary care and into specialized areas, “we had 413 specialist clinics and over 4,000 patients seen in the North, often in their home communities.”
Despite that reach, McKinney points to the structure of the medical system as the main issue to address.
The current system is built around individual work, which McKinney feels is not an effective approach.
“That idea of having a single doctor attached to a single patient is really out the window,” says McKinney. “We have to change our mindset.”
The issue isn’t simply a lack of doctors or nurse practitioners. The primary care team model improves access by giving patients more ways to see a provider and have their needs addressed.
As an alternative, the NMS works around teams. “We work as primary care teams with nurses, nurse practitioners, physicians,” says McKinney. “You’re not relying on one person, it’s not functional, it’s not sustainable.”
The role of “gatekeeper” that primary physicians occupy gets replaced by the support of a well-rounded team.
This approach is reflected in programs for reserves and remote communities. Referrals are replaced with earlier assessments through schools and community-based care, while specialists are brought directly into communities.
While this approach is on the look for expansion, not all of Saskatchewan can benefit from it.
When primary care is limited and out of reach, emergency rooms become the first and sometimes the only option for many rural and First Nation patients in Saskatchewan.
Gail Boehme, executive director of the All Nations Healing Hospital, says the facility serves a large and diverse area including rural residents, and as a result the demand for services continues to increase.

Emergency Entrance at All Nations Healing Hospital. Photos by Andrea Vera.
“Our hospital sees over 10,000 ER visits a year,” Boehme says, noting that the hospital is one of the busiest rural facilities in southeastern Saskatchewan.
In 2024-25, All Nations Healing Hospital (ANHH) experienced sustained high ER volumes and acuity, and frequent EMS bypasses due to staffing shortages and aging x-ray equipment downtime.
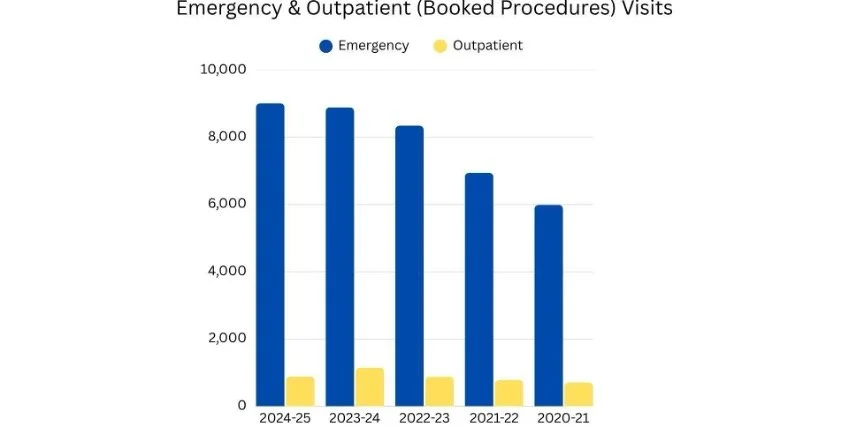
In 2024-25, All Nations Healing Hospital (ANHH) experienced sustained high ER volumes and acuity, and frequent EMS bypasses due to staffing shortages and aging x-ray equipment downtime. Data from AHH 2024-25 Report Graph by Deborah Adedayo.
The graph illustrates emergency room visits at the hospital over time, showing consistently high patient volumes and reinforcing how limited access to primary care is driving more people to rely on emergency services.
High patient volumes reveal a deeper issue within the province’s health system. Limited access to family doctors pushes more people into emergency departments for care that could have been treated earlier.
The growing reliance on emergency departments for non-emergency care highlights the gaps in access to primary healthcare. Boehme explained that many patients turn to the ER because they lack consistent access to primary care providers such as family doctors.

Emergency Entrance at All Nations Healing Hospital. Photo by Andrea Vera.
“There is an overrepresentation of First Nations people in emergency departments,” she says. “That is because there is also an underrepresentation in ability to access primary care.”
The imbalance in healthcare suggests this is driven by multiple barriers, including discrimination, racism, limited availability of physicians, and negative experiences within the healthcare system.
Many patients turn to emergency rooms because their conditions are immediately life-threatening and they have no alternative.
As a result, emergency departments are increasingly functioning as substitutes for family doctors in underserved communities.
Boehme also points to broader system pressures, including emergency room closures in nearby communities such as Melville and Indian Head.
These closures place additional pressure on remaining facilities, forcing hospitals like All Nations Hospital to take in more patients while advocating to maintain their services.
Boheme’s perspective also underscores the broader reality facing rural Saskatchewan, without improved access to primary care, emergency departments will continue to carry the burden of a system.
The struggles around accessing care are not isolated. Dana Henderson is also a resident of Pasqua First Nation. As a nurse practitioner at the All Nations Hospital and more recently as a mother, she has witnessed the lack of primary care from a different perspective.

Danna Henderson. Photo contributed by Danna Henderson.
“It wasn’t until I became a mother, that I started to encounter the healthcare system in a different manner,” says Henderson
Her daughter, 15-year-old Danna-Lee was born with a congenital birth defect, magnifying the struggles of having to find primary care outside their reserve. "My journey began there, since her birth,” says Henderson.
The reserve has the Circle of Care Centre, where only a physician and a paediatrician come in monthly, however, access is never straightforward. Historical realities still create hesitation for Indigenous people to access different services.
Circle of Care Centre at Pasqua First Nation. Photo by Andrea Vera.
“People don't utilize the services because they're scared of confidentiality,” says Hendersen. “They're scared of people saying what they’re doing there and that's why they travel so far too.”
While the drive to the closest primary care clinic at the All-Nations Hospital is from 15 to 20 minutes, mistrust and systemic issues create different barriers to access care.
“A lot of us suffer in silence and pain. In my case, my mother prefers to go to Melville, which is a little over an hour away from our nearest hospital, and that shouldn't happen,” says Henderson.
Henderson’s combined experiences had led her to do advocacy work. In the summer of 2025, she wrote an advocacy report towards the All-Nations Hospital, after a physician dismissed and misdiagnosed her mother’s medical complications.
“It really got me upset because they didn't look at her as a human being,” says Henderson. “My passion for nursing and my passion for advocating, that's what resulted out of it.”
The need for patient advocacy is not exclusive to Henderson. With many people in need of advocacy services, the First Nations Health Ombudsman Office (FNHOO) was established in 2023.
Since being in operation it has received 391 complaints and resolved 224 of them. Complaints the FNHOO hears include the lack of access to physicians, hospitals and emergency rooms, with many coming from Northern Saskatchewan.
The following graph demonstrates the FNHOO’s most commonly heard complaints:
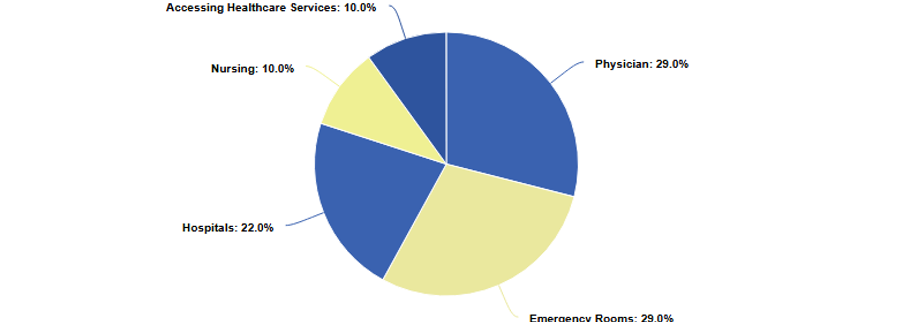
This graph shows the most common complaints that the FNHOO hears. Out of the 391 complaints received, the two most commonly heard involve situations with physicians or in emergency rooms.
With only a few clinics available in the province, many rural residents across Saskatchewan also experience barriers to access primary care.
Student Lizzie Mckay, who has lived in both Weyburn and Melville, has spent her life dealing with difficulties in receiving medical help.
Mckay believes healthcare in rural communities isn’t what it used to be.

Lizzie McKay. Photo contributed by Lizzie McKay.
Mckay says finding a family doctor feels “pretty much impossible these days.”
"I haven't had a consistent doctor since I was six," says Mckay.
Since her early childhood, her parents struggled to connect with a consistent family physician. For most people in that position, the idea of a "local" clinic is non-existent.
For her and many people in rural Saskatchewan, travelling is an additional barrier to getting consistent care.
“Most families just can't afford the time or gas (for a) one day trip for a quick family doctor visit,” says McKay.
At the Melville clinic, McKay says the wait times were “so long (that) some people aren't even being seen”
“I know the staff are trying the best they can, but it just feels like the whole system is broken down,” she says.
She added that sitting in waiting rooms can feel pretty desperate, and how people have to wait for hours with no guarantee of being seen.

Weyburn General Hospital. Photos by Connolly Gamble.
One of the biggest problems is disconnection, rooted in jurisdictional issues. Mainly the bridging gap within health data systems, even when patient information exists.
Provincial systems access data from First Nations communities when justifying funding requests.
“A lot of First Nations communities are quite frustrated when their data is being used,” says McKinney. “Reserves don't get the funding, the SHA (Saskatchewan Health Authority) gets the funding.”
Dr. Udoka Okpalauwaekwe, a physician and primary care researcher at the University of Saskatchewan, emphasized that the lack of data is one of the biggest barriers within the healthcare system.
“We don’t have a standardized, integrated data repository,” says Okpalauwaekwe. “What we have are snippets of studies, people doing surveys, making scientific guesses.”
On March 18, Saskatchewan released its 2026–27 provincial budget. Health Minister Jeremy Cockrill announced record health spending of $8.5 billion, an increase of $393 million, describing healthcare as the largest area of investment in the province.
“The biggest impact that you’re going to see around primary care access in rural Saskatchewan is really around some of the nurse practitioner initiatives,” says Cockrill.
The budget also introduces a $1 million virtual care pilot, targeting communities with low access to primary care providers.
“The frustrations come from not having enough staff, having to work overtime,” Cockrill says.
“How do we address that? We have more staff.”
McKinney says the implications of the Saskatchewan Government investment on the Patients First plan, which prioritizes nurse practitioner’s recruitment and the expansion of Virtual Care.
“Nurse practitioners are very good, but they’re only one part,” says McKinney. “Just like a physician is one part, you need the whole team.”
She also adamantly pushed back on the idea that virtual care can replace in-person services, “It should be an adjunct, like talking to family on the phone in between visits,” says McKinney.
Looking ahead, Gail Boehme, executive director of the All Nations Healing Hospital, believes we need to rethink how services are delivered.
“If we can improve healthcare for the most challenged individuals, you improve it for the entire population,” says Boheme, “To be able to improve it, we need to have it accessible.”
Similar to Boheme, McKinney argued that any real solution has to begin with respect for First Nations communities and their right to define what they need.
“We need to stop treating our First Nations communities as if they don’t know what their needs are,” McKinney says.
“In a perfect world, it would be perfect to have a doctor and a physician to go out to the nation at least twice a week to go see the people that can't travel off the nation,” says Peigan.
For Peigan the solution is straightforward, physicians need to be present on reserves and in every community. Something Peigan says everyone who desperately needs a doctor hopes for each day in this province.